Couples who want to study their irregular menstrual cycles and their difficulties with pregnancy first need to examine the two hormones, which include estrogen and progesterone. People believe that prolactin functions as an essential hormone for the reproductive system of women because they associate this hormone only with breastfeeding. However, prolactin and fertility in women are closely connected, and an imbalance can lead to serious reproductive issues.
Prolactin production in women starts after childbirth through the brain's base, which creates this hormone and the pituitary gland, which acts as the body's main source of this hormone. Women who are not nursing their babies can find prolactin in their bodies because it exists in measurable amounts during their entire reproductive lifespan. Women show regular prolactin levels that begin from specific age points in their lives until they reach their reproductive age. Women lose their ability to ovulate and become pregnant when their prolactin levels rise above normal. This is how high prolactin levels and ovulation are directly linked.
Hyperprolactinemia represents a medical condition that leads to elevated prolactin levels. Doctors frequently overlook this condition because it serves as one of the main medical causes that lead to infertility in women. Prolactin functions as a hormone that increases its levels in the body, but this process creates obstacles for women to achieve their goals of becoming pregnant.
Prolactin exists as a polypeptide hormone that lactotroph cells in the anterior pituitary gland produce and release into the bloodstream. The body of pregnant and postpartum women produces higher prolactin levels because this process enables them to breastfeed their babies through milk production, which serves as a natural biological function.
The prolactin levels normal range in women exist outside the period of pregnancy and breastfeeding. Non-pregnant women maintain prolactin levels that range from 2 ng/mL to 29 ng/mL, although different laboratories have different reference ranges. The normal range of levels for men extends from 2 ng/mL to 18 ng/mL.
Most people do not realize that increasing the prolactin levels will induce the immune system activity, along with affecting metabolic and emotional states. Prolactin functions in human reproduction because its normal levels must remain below specific thresholds, which allow menstrual cycle hormones to function properly.
The problems start when prolactin levels increase beyond their typical limits. An elevation in hormone levels brought about by hyperprolactinemia ultimately leads to a full halt of ovulation, clearly explaining how high prolactin affects ovulation.
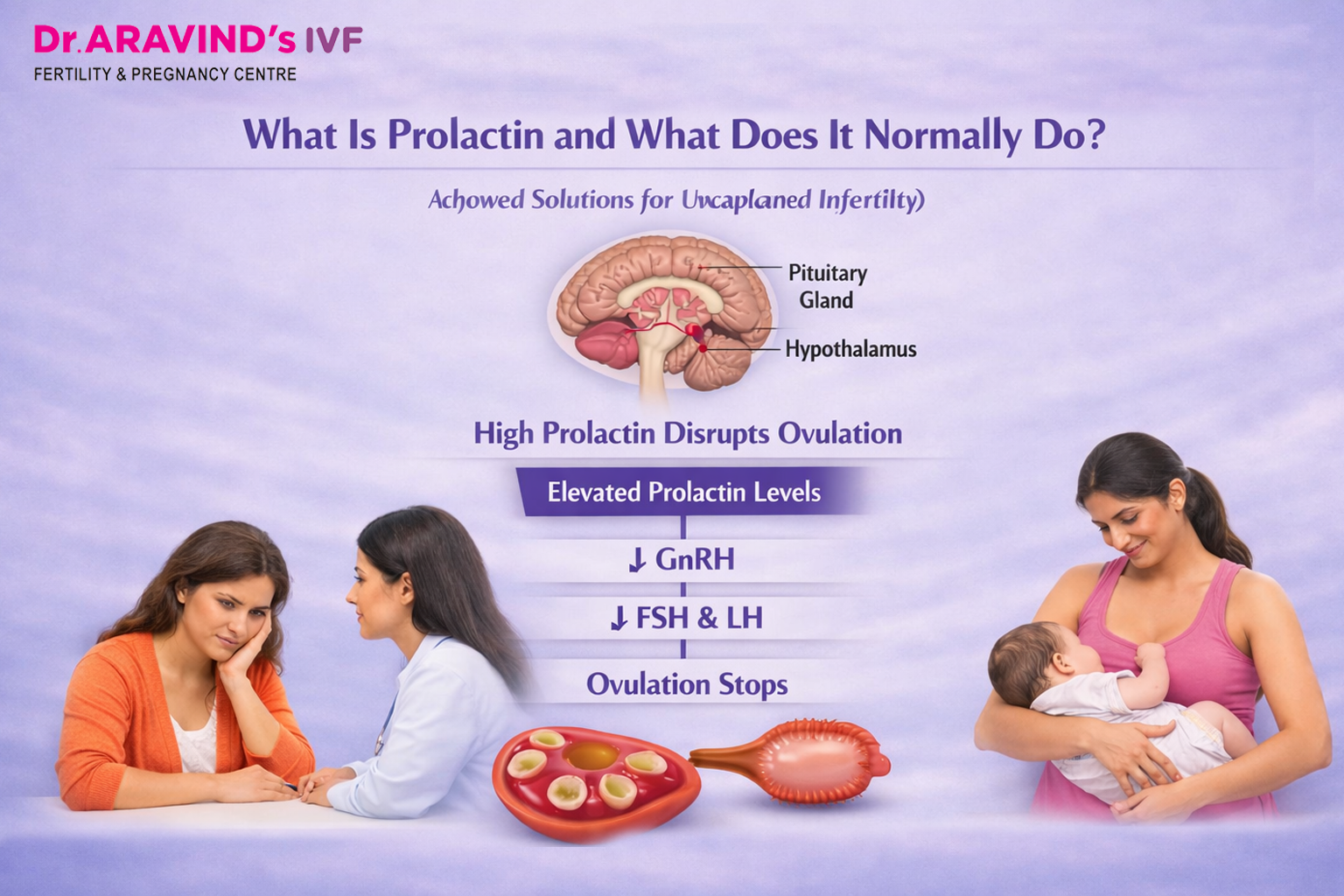
Scientists need to study the triggers of ovulation because they need to understand how elevated prolactin levels disrupt fertility research. The pituitary gland releases Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH) to control the process of ovulation. FSH causes ovarian follicles to grow and develop, but an increase in LH triggers the release of a mature egg, which starts ovulation. The hypothalamus produces Gonadotropin-Releasing Hormone, which controls the secretion of both FSH and LH from the pituitary gland.
Prolactin levels rise above normal limits, which leads to suppression of GnRH release from the hypothalamus. The reduced GnRH level causes the pituitary gland to decrease its production of FSH and LH. Follicles require FSH to undergo correct development. The lack of an LH surge prevents the occurrence of ovulation.
An ovulation occurs when women stop ovulating their menstrual cycle. A woman without ovulation cannot achieve pregnancy because there will be no egg available for fertilization. The body needs LH to produce progesterone after ovulation, but its absence interrupts this process, which leads to menstrual cycle disturbances and reduced uterine lining capacity to support a potential pregnancy.
Women in this situation experience either oligomenorrhea, which causes infrequent periods or amenorrhea, which leads to complete period absence, or they develop irregular cycles. These are common symptoms of high prolactin in females.
Hyperprolactinemia has many possible sources, and medical professionals must identify its precise origin before they can determine optimal treatment methods. Here are the most frequently encountered causes:
A prolactinoma is a pituitary gland tumor which produces excessive prolactin because it is a benign (non-cancerous) growth. The most common medical condition causes elevated prolactin levels. Prolactinomas are classified as microprolactinomas, which measure less than 10 mm and macroprolactinomas, which measure more than 10 mm. Most of the cases can be managed through medication rather than needing surgical interventions. This condition is strongly associated with prolactinoma and fertility issues.
The underactive thyroid gland releases Thyrotropin-Releasing Hormone (TRH), which triggers the production of thyroid-stimulating hormone and prolactin. This is why thyroid function is routinely evaluated in women with elevated prolactin.
Several medications that doctors frequently prescribe to patients produce an effect that leads to increased prolactin levels. Antipsychotic drugs include risperidone and haloperidol, while certain antidepressants and antiemetics, such as metoclopramide and specific blood pressure medications, also contribute to this effect. Your fertility specialist needs to know if you take any of these medications.
People experience temporary increases in prolactin levels when they deal with physical and emotional stress. Prolactin levels will rise above their normal range because of vigorous exercise, inadequate sleep and extreme psychological pressure. The medical field requires multiple tests to confirm a diagnosis because a single abnormal test result needs to be retested.
Prolactin levels in women with PCOS show mild elevation, which does not represent the main hormonal disturbance of their condition. The hormonal environment of PCOS creates a feedback loop that makes ovulation more difficult for women who have this condition.
Women experience increased prolactin levels when they experience mechanical stimulation of the breast or nipple area through clothing friction, chest surgery or self-examination.
Some women develop hyperprolactinemia, which does not have a known cause after their medical evaluations are complete. This condition is known as idiopathic hyperprolactinemia. The medical treatments will work effectively for these women.
Hyperprolactinemia does not always announce itself loudly. Some women experience all possible symptoms, while others can only identify their condition after they face problems with conception. The most commonly reported symptoms include:
The statement explains that not all women with high prolactin levels will experience nipple discharge or show a complete absence of menstrual cycles. The condition causes women to experience ongoing menstrual periods while they fail to produce eggs, which remain undetectable until doctors perform particular examinations.
Your fertility doctor will conduct a prolactin blood test because you have shown symptoms of pregnancy issues, and you have been trying to conceive for several months. The blood draw is usually performed in the morning because prolactin levels reach their highest point during sleep and after a person wakes up. The test should be conducted after fasting because food, nipple stimulation and stressful situations will cause temporary increases in test results. The test result will show heightened prolactin levels, so the medical staff will conduct a second test on a new date to verify results. The medical team will conduct research to find medical problems after they discover a person has constantly elevated levels. The investigation process will involve the following procedures:
The Dr. Aravind IVF centre operates as a full-service fertility center which provides couples with quick diagnosis results that enable the immediate start of their treatment process.
The positive aspect of hyperprolactinemia shows that it stands as one of the easiest hormonal infertility reasons to treat successfully. Many patients benefit from prolactin treatment for infertility, which helps restore ovulation. The identification of the cause permits doctors to administer specialized treatment, which most women will respond to because their ovulation cycle will begin again within weeks or months after treatment starts.
Dopamine agonists represent the primary medication group that doctors use to treat patients with hyperprolactinemia. The brain produces dopamine, which acts as a natural prolactin inhibitor, while these medications function as dopamine receptor binders that operate within the pituitary gland to decrease prolactin production.
The two most widely used dopamine agonists are Cabergoline and Bromocriptine. The medical community now favours Cabergoline because it requires patients to take medication twice a week, which results in fewer side effects while most patients achieve effective prolactin decline. Patients taking Bromocriptine, which is taken once a day, can use this treatment because it has been proven safe for both pregnant women and their unborn children during its extended period of use.
Most patients will experience a decline in their prolactin levels between two and three weeks after they start receiving medical treatment. The process begins when prolactin levels decrease because it allows the body to produce GnRH while FSH and LH levels increase to their correct levels, which enables normal follicle development and subsequent ovulation.
The thyroid condition requires levothyroxine treatment because hypothyroidism causes an increase in prolactin, which will resolve after this medication. The physician who provides treatment for the patient will examine other medication options that have a reduced possibility of causing prolactin elevation, at which point the situation allows for such assessment.
The treatment of prolactinomas requires surgical intervention only in exceptional situations. Most patients with larger tumours respond positively to dopamine agonists. The medical procedure of transsphenoidal surgery permits doctors to eliminate pituitary tumours when all other treatment options have failed, or when patients cannot handle the medications or when the tumour actively endangers their eyesight through optic nerve compression.
After their prolactin levels return to normal and their ovulation processes resume, many couples achieve successful natural conception. Patients who experience other fertility issues, like male infertility, blocked tubes, endometriosis or low ovarian reserve, should think about undergoing extra fertility procedures.
Dr. Aravind's IVF provides customized treatment programs for every patient. The medical team will conduct a complete partner evaluation after treating hyperprolactinemia to make sure they have addressed every potential cause. The medical services provide three treatment options, which doctors select for their patients based on specific medical needs. The three available treatment options include ovulation induction, IUI, IVF and ICSI
The treatment of hyperprolactinemia relies on a doctor’s prescription of medications, yet patients can achieve better treatment outcomes through their implementation of particular lifestyle modifications.
For over 30 years, Dr. Aravind's IVF Fertility & Pregnancy Centre has been an early adopter in reproductive medicine. The network provides advanced fertility services to thousands of families through its centres, which operate throughout Tamil Nadu, Karnataka, Kerala, Andhra Pradesh and Sri Lanka.
Dr. Aravind's IVF Fertility and Pregnancy Centre distinguishes itself through its combination of contemporary medical technology and its commitment to providing personalized patient care in a compassionate manner. The clinic provides each couple who arrives with complete assessments and clear treatment pathways and emotional assistance throughout their entire process.
The centre demonstrates its expertise through more than 70,000 completed IVF cycles, which achieve a 75 percent success rate for live births. The team at Dr. Aravind's IVF possesses all the necessary resources and skills to assist you in achieving your parenting goals through either simple hormonal treatment or advanced reproductive technologies.
More people think that high prolactin levels occur in less than the actual frequency, which proves incorrect because these levels appear in much higher amounts. The hormonal cascade, which starts with elevated prolactin levels, will create complete ovulation suppression, which transforms natural pregnancy processes into challenging emotional situations.
Health specialists can determine the presence of hyperprolactinemia through a blood test, which physicians can use because they know all the factors that cause the condition, and the available treatments show reliable success rates. Most women with high prolactin levels can achieve normal hormonal function through appropriate medical treatment, which enables them to restore their ovulation process before they become mothers. With proper diagnosis and the right prolactin treatment for infertility, most women can restore ovulation and achieve pregnancy successfully.
People should seek immediate medical assistance when they experience hormonal issues that lead to irregular menstrual cycles and difficulty achieving pregnancy, or when they need to check their current hormonal status. You need to contact a trained fertility specialist who will perform an in-depth hormonal assessment of your condition.
Yes, high prolactin suppresses GnRH hormone release, which reduces FSH and LH levels. This prevents ovulation, making pregnancy difficult.
Common symptoms include irregular periods, missed periods, infertility, nipple discharge (galactorrhea), low libido, and vaginal dryness.
Pregnancy is difficult but possible. However, most women need treatment to restore ovulation and improve fertility chances.
Causes include prolactinoma, hypothyroidism, medications, stress, PCOS, and sometimes unknown reasons (idiopathic).
Treatment typically involves dopamine agonists like cabergoline or bromocriptine, along with treating underlying conditions such as thyroid disorders.
